
Neurotech moonshot
Approach for making the general-purpose brain-machine interface happen

‘We choose to go to the moon. We choose to go to the moon in this decade and do the other things, not because they are easy, but because they are hard, because that goal will serve to organize and measure the best of our energies and skills, because that challenge is one that we are willing to accept, one we are unwilling to postpone, and one which we intend to win, and the others, too.’
President John F. Kennedy at Rice University, Houston, Texas, 1962.
A seminal paper on brain-computer interfaces was published a little over fifty years ago, in June 1973 [1]. In this paper, Jacques Vidal coined the term ‘brain-computer interface’ [2] and concluded that ‘... direct brain-computer communication still lies somewhat in the future.’[1]
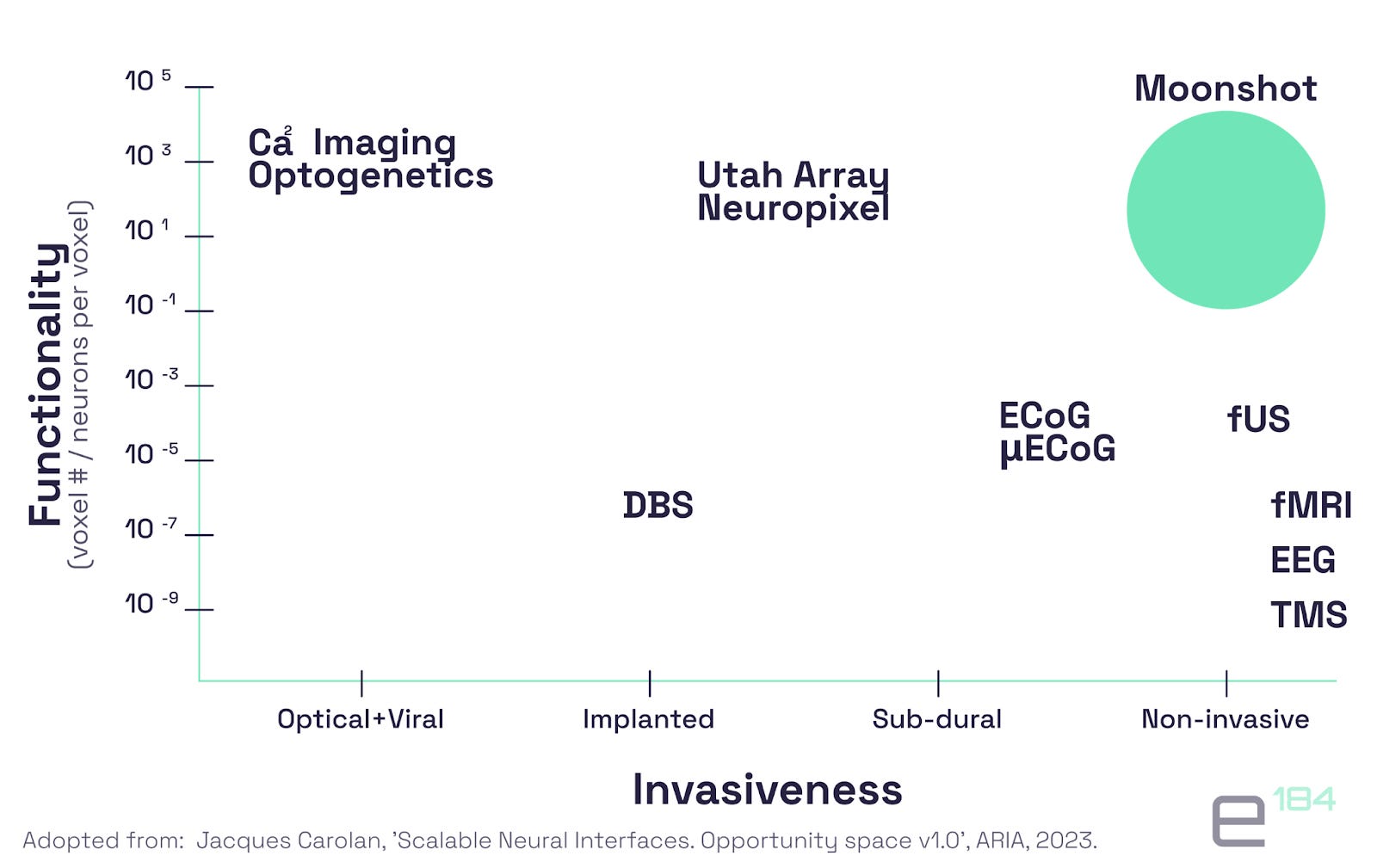
Having tried a good chunk of existing neurotechnologies on ourselves (tDCS, EEG, MEG, fNIRS, fUS, to name a few) and researched many more, we recognise the astonishing progress in the field: speech and image decoding [11,12], evoking visual sensations [13] for example. But we must admit that Vidal’s future, our present, did not bring direct brain-computer communication. The neurotech field itself remains in its infancy. Its fragmentation and low technology adoption rate indicate how young neurotech is. The most advanced technologies are still confined in laboratories and hospitals and require implantation (see a chart below).
No common language and limited adoption
The narrative and language of neurotech remain fragmented. For instance, there are still ongoing debates about the distinction between brain-computer interface and brain-machine interface [14,15] and about terminology around invasivness levels [16]. For example, whether the definition of the brain implant should be based on to what extent ‘... acquired data remains “internalized” to drive tissue stimulation or is extracted to drive an external artefact’ or based on ‘the safety during implantation and operation’ [14].
Even if several definitions might be complementary, to grow, and translate into the clinics or daily lives of the general public, the neurotech community will have to agree on the dominating approach to better communicate with investors, industry, and the general public. We follow the BMI definition, as it implies a wider list of technologies to communicate with and allows for a surgical system.
Applications of neurotech remain niche and not widely adopted. Excluding a couple of laser-focused applications (cochlear implants, deep brain stimulation - DBS), neurotechnologies are nowhere near their peers from other fields in terms of adoption. For example, probably the largest non-invasive neurotech developer, Muse, scores five hundred thousand users [4], while Apple sells thirty to fifty million watches annually, and they are a class II medical device [5]. On a more invasive front, half a million Americans undergo Lasik surgery every year to correct their vision [17], while even the most mature neurotechnology, DBS, scores ca. twelve thousand surgeries per year [19].
General-purpose vs applications
Our intuition is that limited neurotech adoption results from overemphasising applications at the expense of developing general-purpose technology/platform (we use these concepts interchangeably for simplicity). Using Benjamin Reinhardt’s metaphor [18], building frontier tech is akin to cave diving. The end goal is remote and not clearly seen, so the trajectory to reach it should be carefully planned. Air pockets (tech ‘exit ramps’, temporary applications) along the route should be selected in a way that minimizes diverts from the final destination. When ‘air pockets’/immediate applications are overemphasised, one is stuck with them, and the end goal becomes unattainable.
We saw the consumer neurotech wave in the early 2010s, when venture capitalists poured money into tech that underpinned what they expected to be neurotech killer features, such as focus or sleep enhancement. Aiming for faster traction, consumer neurotech pioneers underinvested in research and initiated design freezes too early, when, for example, a headset had sensors optimally located for a particular application but not well-positioned for expansion to other applications. As a result, the consumer wave produced some outstanding companies, but they remained niche, and the field itself did not really enter the daily lives of most people.
Now, we are witnessing a trend towards neurotech absorption by medtech. Since some of us fell in love with neurotech following family health tragedies, we appreciate medical technologies and admire researchers and entrepreneurs who solve healthcare. However, diving into medtech and losing sight of the general-purpose tech will lead to results that are not dissimilar to the consumer neurotech wave a decade ago. We are sure that some of the most pressing healthcare challenges will be solved by neurotech, and medical neurotech behemoths will be created, but we are not sure that this will bring the general-purpose BMI closer.
Building a medical rather than a general-purpose product is different in many respects. To name a few, neuromodulation, probably the most required capability for medical success, might not be necessary for a consumer product, and requirements for medical devices that address patients' comorbidities could probably be loosened for healthy users.
Founding and funding a general-purpose BMI
A moonshot approach to neurotech focuses more on developing general-purpose tech rather than immediate applications, it also emphasises scalability and frictionless of the system, either through its non-implantable nature, or smooth implantation process.
In the cave-diving paradigm, funders (private investors, philanthropists, or otherwise) and founders are less concerned with selecting the ‘silver bullet’ niche/a killer app but care more about picking ‘... an “optimal” sequence of niches or searching around for yet-unknown niches instead of being forced to hop into the nearest or most obvious ones’ [18]. Our approach to neurotech is that all current applications are rather a sequence to the ultimate BMI platform.
Space tech is an excellent example of applying this cave-diving metaphor. A remote moonshot goal, such as a lunar landing for the Apollo mission or bringing humans to Mars for SpaceX, was decomposed into more achievable missions with interim tech feedback loops and even some market feedback in the case of SpaceX. The Gemini programme offered multiple ‘air pockets’ required to make Apollo a reality [21]. Elon Musk charted a path to his moonshot (marsshot?) through NASA-subsidized LEO rocket, GEO rocket, reusable GEO rocket, and finally Starship [18].
To enable experimentation and focus on general tech instead of applications, e184 draws inspiration from the advanced research project agencies (ARPAs, defence ARPA — DARPA being the most famous) and focused research organisations (FROs). Focus on experimentation and general tech means that we lean towards imaging and decoding technologies, even if they are not linked to immediate applications, unlike many neuromodulation technologies, for example.
Where will the general-purpose BMI come from
We are very excited about several lines of research and engineering enquiry, among them are:
minimisation of risks and frictions associated with existing single-neuron resolution decoding systems (microelectrode arrays - MEAs, depth probes, similar to Neuropixel, flexible electrodes);
pushing the boundaries of non-implantable systems, including those that decode directly from neuron activity (MEG, EEG, to name a few) or indirectly from the brain’s hemodynamics (fNIRS, fUS, for instance);
developing new modalities that have not been significantly or at all tried in human subjects, like optogenetics or neural dust, for example;
exploring how progress in basic science could accelerate BMIs, e.g., by identifying new areas for speech decoding or new ways of manipulating atomic vapour contained in the glass cells of OPM MEG units.
Focusing on these lines of work and decoupling them from the market and applications will not be easy due to the dominant incentives paradigm. Regulators, for instance, the United States Food and Drug Administration (FDA), emphasise clinical indications when granting Premarket Approval (PMA), 510(k) clearance, or, to a lesser extent, Investigational Device Exemption (IDE). Private investors expect traction with payors and, therefore, achieve clinical benefits.
Obtaining regulatory approval as a tool, rather than medical devices for end users, becomes a viable option for BMI developers. For instance, numerous electrocorticography (ECoG) systems achieved FDA clearances and/or CE marks for use in patients during intraoperative neurophysiological monitoring in neurosurgery [20]. Remaining a professional tool, even within the limits of specified indications, allows for the avoidance of overspecialisation required by a medical device that is available to end-users.
Luckily, alternative funding options are emerging that focus less on immediate commercialisation. In addition to government agencies like DARPA, private ARPAs and new philanthropy options like FROs have emerged.
We aim to provide patient capital and support to allow entrepreneurial scientists to discover and build a new generation of BMIs. We also aim to become a sounding board and a sparring partner for entrepreneurs, someone who may help maintain focus during the long journey without an immediate application in sight.
With an extended catalogue of funding options available and emerging regulatory pathways, we think it’s time to choose a moonshot and focus on the general-purpose brain-computer interface.
We invite you to join us on this journey and share your thoughts and questions: subscribe and contact Peter (p@e184.com).
References
[1] https://www.annualreviews.org/content/journals/10.1146/annurev.bb.02.060173.001105
[2] https://www.nytimes.com/2022/05/12/magazine/brain-computer-interface.html
[3] https://pubmed.ncbi.nlm.nih.gov/32164849/
[6] https://www.peterzhegin.com/investor-notes-from-the-fields-of-the-neural-interfaces-summit/
[7] https://www.cnbc.com/2024/06/21/paradromics-gears-up-to-test-its-brain-implant-on-humans.html
[10] https://www.from-the-interface.com/DARPA-funding-BCI-research/
[11] https://www.nature.com/articles/s41586-023-06443-4
[12] https://arxiv.org/html/2404.05468v4
[13] https://www.pnas.org/doi/10.1073/pnas.1713447114
[14] https://www.nature.com/articles/s41467-024-50603-7
[15] https://bcisociety.org/bci-definition/
[16] https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2021.599549/full
[17] https://www.theguardian.com/us-news/2023/apr/18/lasik-laser-eye-surgery
[18] https://benjaminreinhardt.com/parpa
[19] https://my.clevelandclinic.org/health/treatments/21088-deep-brain-stimulation
[20] https://www.tandfonline.com/doi/full/10.1080/17434440.2024.2343421#abstract
[21] https://history.nasa.gov/wp-content/uploads/static/history/alsj/GeminiSummaryConf_SP-138.pdf